Academic report “Understanding the Role of Internet Access on Health and Health Equity toward Healthy Ageing in the Western Pacific Region” published.
We are pleased to announce the release of a new academic report on the relationship between Internet access and health among older adults in Japan and Myanmar. The results of the analysis in the report was all shared with WHO Western Pacific Regional Office. This research report contains the results of our research conducted in Myanmar in 2018 before the military coup. All JAGES members hope that the situation in Myanmar will normalize as soon as possible.
Here is the executive summary of the report.
----------------------------------------------------------------------------------------------------------
EXECUTIVE SUMMARY
Digital technology is gaining great importance as a health tool in today’s world, especially in the wake of the COVID-19 pandemic. The lockdowns during the pandemic have highlighted how important access to online services is for vulnerable populations, especially older people. Thus, it is crucial to examine the level of digital access enjoyed by older people from different socio-economic groups and provide robust evidence on the issue. Often, it has been said that older people are likely to have limited access to digital devices and the Internet because of their biological (e.g. impaired mobility, eyesight, cognitive function, and mental health) and social (e.g. low income, isolation, and social exclusion) disadvantages. Since Japan leads the world in longevity and growing older population, we are in a position to provide the required evidence.
Using cross-sectional (data at a specific point in time) and longitudinal (follow-up data) data from 40 municipalities in nationwide Japan, and cross-sectional data from two local regions in Myanmar. This report finds evidence of a strong association between frequent Internet use and good health and well-being, mainly low depression risk, high self-rated health, greater capability for activities of daily living (ADL), and well-connected social relationships from Japanese data. Notably, these associations were not affected by income, educational attainment, or other socio-economic factors.
We provide clear evidence of the digital divide among older people belonging to different socio-economic groups and/or residential regions. In Japan, the Internet was used by half of the older population. However, older people with higher income and more educational attainments were more likely to be frequent Internet users (Figure 1).
Internet users were found to be more socially active compared to non-users (Figure 2). Those who used the Internet almost daily used it for shopping and banking, indicating that Internet use helps older people perform these two essential activities in their daily lives. Additionally, Internet use lowered the risk of depression by about 40% among those who were at a high risk for developing depression due to their socially disadvantaged background. (Figure 3)
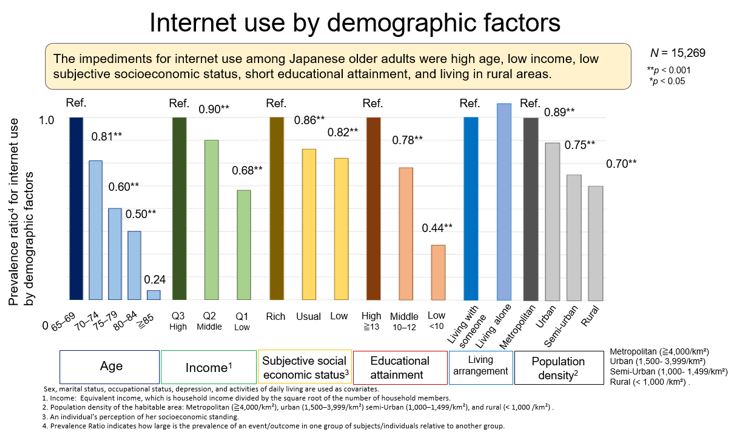
Figure 1. Characteristics of Internet access among Japanese older people (page 51)
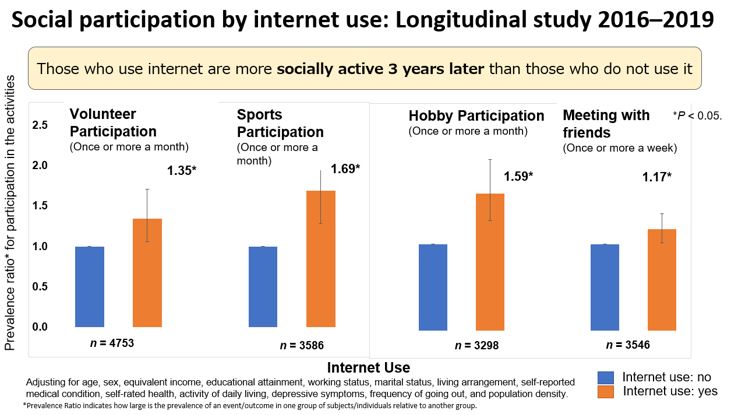
Figure 2. The association between Internet use and social participation after 3 years (page 43)
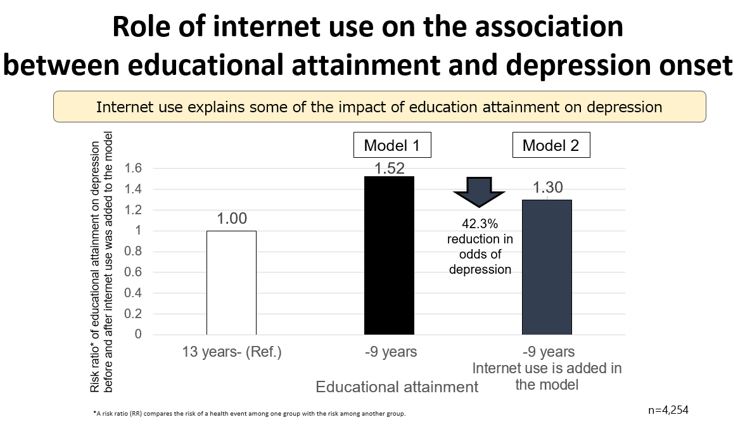
Figure 3. Internet use explained the associations between educational attainment and depression onset by 42% (page 54)
Evidence from a city (Yangon) and a rural area (Bago) in Myanmar shows trends of a digital divide possessing similar to those seen in Japan: good socio-economic conditions or urban setting were linked to Internet access and Internet users had better health. Moreover, a huge gap in Internet access may exist between the urban and rural population in Myanmar.
Figure 4. Findings of this study (page 85)
In the face of compelling evidence on the existence of a digital divide in the older population, bridging this divide should be a priority of policymakers. Our findings confirm that reducing the digital divide can contribute to fostering health equity among older adults. This report is only the first small step in unravelling the complex picture of the digital divide among older people, and we hope that future studies will be able to find the mechanism linking Internet access, socio-economic status, and health and well-being among older adults residing in the Western Pacific Region. (Figure 4)
Figure 5. Policy implications (Page 87)
Further, we encourage future studies to apply more advanced causal inference models along with rich and high-quality data from Japan, Myanmar, and other countries to ascertain the causal role of Internet use in the health and well-being of older people. More solid evidence is desired from the future survey and study in the other Asian countries including Myanmar. We urge other researchers to study the effect of Internet use on various health outcomes as well as mortality and onset of medically diagnosed diseases using data from official health reports, while also taking into account various social factors affecting health. We also urge them to investigate links between Internet use, socio-economic status (SES), and healthcare systems to understand the complex picture of Internet use and older people’s health and well-being. Such comprehensive understanding of the issue would help design effective interventions, such as providing resources to older people or improving their digital literacy, so that all older people, irrespective of socio-economic status, can enjoy the health benefits resulting from Internet use.
Our society is rapidly transitioning to a digital world and this transition was accelerated by the global COVID-19 pandemic. As Internet use becomes more and more essential in our day-to-day lives, people left behind in the digital wave are likely to face many disadvantages, physically, mentally, and socially. The evidence we provide of the divide in digital technologies and health among older people is a stepping-stone for future studies to investigate public health problems emerging from the aftermath of the current pandemic at local, national, and global levels.
Understanding the role of Internet access on health and health equity toward healthy ageing in the Western Pacific Region/ Naoki Kondo, Chie Koga and Yuiko Nagamine (Editors). Ver.1.1.
ISBN 978-4-9910804-3-2
Version 1.1. Minor description correction, Published on 14. Sep. 2021
Version 1.0. Published on 26. Aug. 2021
Suggested citation. Kondo N, Koga C, Nagamine Y editors. Ota A, Shobugawa Y, Cable N, Tajika A, Nakagomi A, Chishima I, Ide K, Ueno T, Fujihara S, Fujinami Y, Yasufuku Y, and Ando Y. Understanding the Role of Internet Access on Health and Health Equity toward Healthy Ageing in the Western Pacific Region. 2021, ISBN 978-4-9910804-3-2
Contact.
KYOTO UNIVERSITY
DEPARTMENT OF SOCIAL EPIDEMIOLOGY
GRADUATE SCHOOL OF MEDICINE / SCHOOL OF PUBLIC HEALTH
Floor #2, Science Frontier Laboratory
Yoshidakonoe-cho Sakyo-ku Kyoto 606-8501 JAPAN
E-mail:contact@socepi.med.kyoto-u.ac.jp
Japan Agency for Gerontological Evaluation Study (JAGES)
6-3-5 Yanaka, Taito-ku, Tokyo 110-0001, Japan
Email: jages-office@jages.net
ACKNOWLEDGEMENTS
This report, entitled Understanding the role of Internet access in older people’s health outcomes for the Healthy Ageing in the Western Pacific Region, was prepared by Department of Social Epidemiology at Kyoto University and Japan Agency for Gerontological Evaluation Study (JAGES Agency). This report was funded by World Health Organization Western Pacific regional Office.
This study used data from JAGES 2016 (the Japan Gerontological Evaluation Study), JSPS (Japan Society for the Promotion of Science) KAKENHI grant numbers (JP15H01972, JP15H04781, JP15H05059, JP15K03417, JP15K03982, JP15K16181, JP15K17232, JP15K18174, JP15K19241, JP15K21266, JP15KT0007, JP15KT0097, JP16H05556, JP16K09122, JP16K00913, JP16K02025, JP16K12964, JP16K13443, JP16K16295, JP16K16595, JP16K16633, JP16K17256, JP16K19247, JP16K19267, JP16K21461, JP16K21465, JP16KT0014, 19K04785, 20H00557, JP25253052, JP25713027, JP26285138, JP26460828, and JP26780328), Health Labor Sciences Research Grants (H26-Choju-Ippan-006, H27-Ninchisyou-Ippan-001 H28- Choju-Ippan-002, H28- Ninchisyou-Ippan-002, 19FA1012, 19FA2001) from the Ministry of Health, Labor, and Welfare, the Research and Development Grants for Longevity Science from AMED (Japan Agency for Medical Research and development) (16dk0110017h0002, 16ls0110002h0001), the Research Funding for Longevity Sciences from the National Center for Geriatrics and Gerontology (24-17, 24-23), and the Japan Foundation For Aging And Health.
This study used data from the Japan Gerontological Evaluation Study (JAGES, 2019).This study was supported by JSPS (Japan Society for the Promotion of Science) KAKENHI Grant Number (JP15H01972→If necessary, please replace or add your own JSPS grant), Health Labour Sciences Research Grant (H28-Choju-Ippan-002), Japan Agency for Medical Research and Development (AMED) (JP17dk0110017, JP18dk0110027, JP18ls0110002, JP18le0110009, JP20dk0110034, JP20dk0110037, JP20lk0310073, 21lk0310073h0002, 21dk0110037h0003), Open Innovation Platform with Enterprises, Research Institute and Academia (OPERA, JPMJOP1831) from the Japan Science and Technology (JST), a grant from Innovative Research Program on Suicide Countermeasures(1-4), a grant from Sasakawa Sports Foundation, a grant from Japan Health Promotion and Fitness Foundation, a grant from Chiba Foundation for Health Promotion and Disease Prevention, the 8020 Research Grant for fiscal 2019 from the 8020 Promotion Foundation (adopted number: 19-2-06), a grant from Niimi University (1915010), grants from Meiji Yasuda Life Foundation of Health and Welfare and the Research Funding for Longevity Sciences from National Center for Geriatrics and Gerontology (29-42, 30-22, 20-19, 21-20).(If necessary, please add your own grants).
This research was funded by the Japan Agency for Medical Research and Development under the project title: ‘Development of a health equity assessment tool based on a social epidemiological survey of older adults in Myanmar and Malaysia’ (Grant Number 17934739). This research was supported by the World Health Organization Centre for Health Development (WHO Kobe Centre—WKC: K18015) JSPS KAKENHI Grant Number JP19K19472 was also used for research. This work was supported by the MHLW Program, Grant Number JPMH20BA2002.


